Scuba Diving
No stop limits (NSL), No decompression limits (NDL)
An old concept that needs to be nuanced
Réf. CMAS/TC/FC/EN/001
As soon as the first dive tables were created, the concept of ‘no-stop dives’ appeared. Inaccurately, it was called ‘No Decompression Limit (NDL)’, which does not correspond to physiological reality, since each ascent phase causes decompression and therefore desaturation of the neutral gas accumulated during the dive. It is therefore better to talk about ‘No Stop Limits’ (NSL) [1].
Level of DCS risk
The risk of decompression sickness (DCS) during scuba diving depends to a large extent on the charge of the neutral gas (nitrogen, helium) to be desaturated. An approximation of this charge was given as early as 1957 by Hempleman [2] under the name of the Q factor or PrT index. The neutral gas charge is equal to the depth (m) multiplied by the square root of time (min). The use of the square root of time is common in science for diffusion phenomena.
Shield [3] then associated a DCS probability to this neutral gas charge.
Comex [4] complemented this approach by refining the associated risks.
The concept of ‘NSL’ within the same dive table
The concept of NSL was born with dive tables, not dive computers. For the same dive table, it is less 'risky' to dive in the NSL than it is to make mandatory stops.
In the past, many organisations (PADI, SSI, NAUI, etc.) have used this concept to define their training courses. Particularly in areas or countries where divers do not have to undergo medical examinations and dive very infrequently, i.e. 3 to 5 times a year, it seemed sensible to limit dives to the non-compulsory stop zone indicated by a dive table, as well as limiting the maximum depth.
However, many other organisations, including those that are members of CMAS, founded in 1959 by Jacques-Yves Cousteau, have taken a different approach, with more stringent training and medical supervision requirements, making it possible to envisage sport diving with mandatory stops, up to 57 or 60 m in air (120 m for helium-based dives), depending on the country.
Worldwide, the estimated risk of DCS does not appear to be greater for either approach. In both cases, it is in the order of 1 to 5 per 10,000 [5] [6] [7] [8] [9] [10] [11].
The concept of ‘NSL’ loses its validity when used between different dive tables or computers
The development of dive computers since the 1980's/1990's has led to the adoption of desaturation methods based on different sets of Haldanian parameters with specific conservatism depending on the computer.
This has resulted in a significant reduction in the no-stop dive curve to reduce the risk of DCS. The use of Gradient Factors (GF) reinforces this point.
Huggins, Karl E, Dynamics of decompression workshop, Course taught at the University of Michigan, 1992, p. 7.
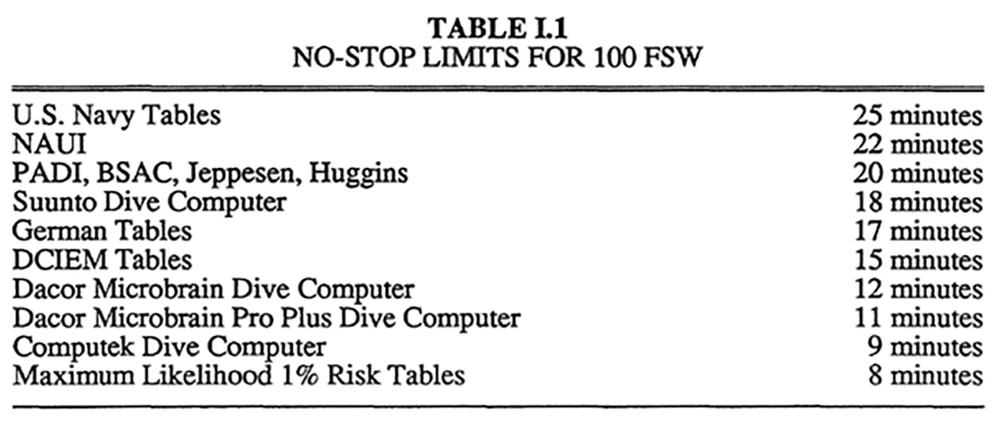
Example of NSL at 100 fsw (30 m). The lower the NSL, the lower the risk of DCS. To dive for 25 minutes at this depth, it is safer to use a computer (or a table) that includes mandatory stops (e.g. Maximum Likelihood 1% risk tables) than to adopt a NSL of 20 or 25 minutes (US-Navy, NAUI or PADI tables, etc.).
As Karl Huggins reminds us in his lecture at the University of Michigan, « If of the many truths you select just one, and follow it blindly, it will become a falsehood, and you a fanatic. Some training agencies dictate which decompression tables should be used by exposing their students to only one of the available tables. If any of the other options are discussed, it is generally in a disparaging light. All this does is to lure newly trained divers in to the false sense of security that the technique they are taught is the "truth." They are not exposed to other theories, models, tables, and debates which exist in the decompression field that are needed to make educated and knowledgeable decisions regarding their own decompression needs. » [12]
CONCLUSION
As a result, today it is better to use sets of parameters that reduce the NSL and to make mandatory stops, than to race for the highest NSL.
We don't think that diving within the NSL should be dogmatic.
The race by some dive computer manufacturers to achieve the highest NSL does not seem to us to be valid, particularly for repetitive dives.
Similarly, the ‘ideology’ promoted by some instructors to their students, demandig ‘as few stops as possible’, seems to us to be a perversion of risk prevention thinking.
More than NSL, risk prevention in diving requires 5 pillars:
- Gradual return to diving;
- Respect for computer instructions;
- Consideration of individual risk factors (hydration, physiological rest, nitrox dives, O2 stops when dives are particularly saturating, 2 to 3 hours interval between dives, physiological rest, etc.);
- Avoid risky profiles (yo-yo, sawtooth, fast ascents, etc.);
- Avoid risky behaviour (Valsalva at decompression, effort after diving, etc.).
Alain Foret
CMAS TC President
REFERENCES
[1] Huggins, K. E., Dynamics of decompression workshop, Course taught at the University of Michigan, 1992, p. 7.
[2] Hempleman H. V., Crocker W. E. and Taylor H. J., Investigation into the decompression tables, Report III, Part A: A New Theoretical Basis for the Calculation of Decompression Tables, Part B: A method of calculation decompression stages and the formulation of new diving tables, Great Britain, Medical Research Council, Royal Naval Personnel Research Committee, UPS, Rept. R.N.P 52/708, U.P.S 131, June 1952, 30 pp.
[3] Shields, T.G., P.M. Duff, and S.E. Wilcox, 1989, Decompression Sickness from Commercial Offshore Air-Diving Operations on the U.K. Continental Shelf During 1982 to 1988, Report produced for Department of Energy (DoE) under Contract #TA/93/22/249. Aberdeen: Robert Gordon’s Institute of Technology.
[4] Gardette B. et Plutarque M., Comex 50 ans de recherches et d’innovations, 2012, pp. 140-142. English version available here (https://www.anciencomex.com/pages/8_la_boutiquepag.html).
[5] Bennett P. B., Epidemiology of decompression illness and fatalities in recreational divers, in Proceeding of the 1st European Consensus Conference on Hyperbaric Medicine, Lille, septembre 1994 ; 28 - 34.
[6] DAN: Divers Alert Network, Annual Report.
[7] Coast Guards, Annual Report, Great Britain.
[8] Enquête annuelle CROSSMED (France), 2003.
[9] Blatteau J.-E., Guigues J.-M., Hugon M., Galland -F.-M., Bilan de 12 années d’utilisation de la table MN 90 par la Marine nationale. Analyse rétrospective de 61 accidents de désaturation, MedSubHyp ; communication présentée lors de la réunion scientifique d’automne de septembre 2004.
[10] Grandjean B., Épidémiologie des accidents de la plongée sous-marine autonome de loisir, in Traité de médecine hyperbare, Ellipse éditions 2002 ; 153 - 159.
[11] Méliet J.-L., coordinateur, Recommandations de bonne pratique pour le suivi médical des pratiquants d’activités subaquatiques sportives et de loisir, MedSubHyp et SFMT, 2020, p.29.
[12] Huggins K. E., Dynamics of decompression workshop, Course taught at the University of Michigan, 1992, p. 8.